


 Reply With Quote
Reply With QuoteOriginally Posted by Jeffrey

My dentist has already shutbthings down for non crises.
Results 2,061 to 2,080 of 22200
-
03-23-2020, 11:07 AM #2061
 Member
Member


- Join Date
- Nov 2007
- Location
- Vermont
my wife finds herself in dental limbo as well, got a temporary crown before the muck hit the fan, now doesn't want to go in any time soon to get the permanent crown put on. Our dentist shut down for two weeks, so he's up to snuff...she's in absolutely no hurry to see him, but has to treat the temporary crown with great dignity and respect, because she doesn't want it to pull off...that's the main threat (don't get gummy bears). Originally Posted by Jeffrey
-
03-23-2020, 11:38 AM #2062
 Member
Member
- Join Date
- Feb 2007
- Location
- Skinker-DeBaliviere, Saint Louis
-
03-23-2020, 11:42 AM #2063
 Moderator
Moderator
- Join Date
- Feb 2007
- Location
- Washington, DC area
I edited your prior post with your fix. Originally Posted by rsvman
-
03-23-2020, 11:57 AM #2064
Member
- Join Date
- Dec 2016
Fixodent that sucker right back up there if it falls out. My temporary crowns never stay in.... Originally Posted by budwom
-
03-23-2020, 12:17 PM #2065
Member
- Join Date
- Mar 2014
Haven't been around in a minute but wanted to check in and say I hope everyone is staying healthy and sane. I'll say for our household that we're mostly healthy.
-
03-23-2020, 12:19 PM #2066
Member
- Join Date
- May 2007
- Location
- Baltimore, MD
Subscribing would be like the Death of the Month club. Originally Posted by golfinesquire
-
03-23-2020, 12:20 PM #2067
Member
- Join Date
- Feb 2007
- Location
- Princeton, NJ
Italy had 18% fewer deaths and 15% fewer new cases on March 22 than on March 21. It's just one day, so hard to know what it means, but it is a welcome change of direction
-
03-23-2020, 12:28 PM #2068
 Member
Member
- Join Date
- Feb 2007
It probably means about as much as all of the other small sample sizes thrown around. Originally Posted by freshmanjs
-
03-23-2020, 12:29 PM #2069
Member
- Join Date
- Mar 2007
- Location
- Asheville
Sadly, I suspect Italy death numbers are not a small sample size. Originally Posted by Indoor66
-
03-23-2020, 12:32 PM #2070
 Member
Member
- Join Date
- Feb 2007
- Location
- Steamboat Springs, CO
Some have trashed our Nobel laureate quoted above for reasoning based on population-wide data in separate countries. As opposed, I suppose, to controlled experiments lab-based results and other more scientifically derived data. As a social scientist, we are used to dealing with messy data that represents a combination of known and unknown effects (that's why it's "social" science, I suppose). Originally Posted by freshmanjs
The point that is being made is that two countries, China and South Korea, which had the disease early, have leveled off in the number of new cases to one percent or less per day of total number infected. Iran also seems to be leveling off. Italy is perhaps an exception, given the large number of cases and the continued growth, but we shall see.
Is COVID-19 going to charge ahead until it infects a high percentage of the population or will it -- better, can it -- be controlled with social distancing and other measures, as well as inherent limitations in its ability to infect everyone?
The China and Korea results are hopeful -- I also "hope" the data are accurate -- the Italy results are more problematic but may, just may, be trending down.
Population-wide studies are messy but can be very informative.Sage Grouse
---------------------------------------
'When I got on the bus for my first road game at Duke, I saw that every player was carrying textbooks or laptops. I coached in the SEC for 25 years, and I had never seen that before, not even once.' - David Cutcliffe to Duke alumni in Washington, DC, June 2013
-
03-23-2020, 12:33 PM #2071
 Member
Member
- Join Date
- Feb 2007
- Location
- Atlanta, GA
Just want to openly thank rsvman, devildeac, et al for your ongoing contributions to this thread. They've been extremely informative and mostly pretty accessible for those of us not in scientific/medical fields.
Also interesting to finally understand what "rsvman" means.
-
03-23-2020, 12:35 PM #2072
Member
- Join Date
- Feb 2007
- Location
- Westport, CT
Just received this email from the academic medical system that I work with:
"We are actively creating a physician continuity plan to deploy in stages as our volume necessitates. We need your assistance in determining the bandwidth of our medical staff. Specifically, who is best-suited and willing to transition their role to a higher level of care. Their role would elevate to either an intensivist or a hospital-based physician (hospitalist). Training programs are in development for this process."
I am an interventional cardiologist. They are asking us to become ICU docs if need be. I'm not sure what to think about this. I certainly can take care of sick "cardiac" patients but I have not managed patients on a ventilator primarily, been primarily responsible to patients with sepsis, viral infections, or any of a host of other critical medical issues in many years (32 years to be exact). While we can get additional "training" I will not be functioning at the level of a board certified intensivist. There will be no blanket protection for me from a malpractice standpoint. I will be more exposed to the virus than I am currently. I will have to leave my office practice and my patients to others during the surge. On the other hand, is it my duty? I feel like my generation got off pretty easily. I missed serving in the Viet Nam war based on age. The first crisis I had to deal with was HIV/AIDS. That was scary for sure, but you knew that you just had to avoid sticking yourself with a needle etc. I felt like we had some control over our protection from HIV. Now, here we are. Time for us to step up. This could be an interesting way to reinvigorate my interest in medicine. Still, I'm torn.
Any others in this predicament?
-
03-23-2020, 12:36 PM #2073
 Member
Member
- Join Date
- Feb 2007
- Location
- Chesapeake, VA.
Thanks. In that case, can you please delete the one in which I quoted myself in an attempt to fix the error? Originally Posted by -jk
"We are not provided with wisdom, we must discover it for ourselves, after a journey through the wilderness which no one else can take for us, an effort which no one can spare us, for our wisdom is the point of view from which we come at last to regard the world." --M. Proust
-
03-23-2020, 12:44 PM #2074
 Member
Member
- Join Date
- Feb 2007
- Location
- Raleigh
You're welcome, but rsvman provides much, much, much better scientific data/education/knowledge/insight than I'm capable of doing. Heck, he's even rebuked me on my ancient/outdated/primitive method of testing for viruses. Originally Posted by wilson

I really had a good LOL a year or two ago when I surmised/found out what rsvman meant.[redacted] them and the horses they rode in on.
-
03-23-2020, 12:53 PM #2075
 Member
Member
- Join Date
- Jan 2010
- Location
- Outside Philly
I think this was directed at my post. My point wasn't to "trash" the guy, rather point out how either he or the article author presented the calculation of growth rate changes as some sort of amazing, new approach. Those calculations are quite literally the input into the curve models. Every day, WHO, CDC, etc are doing those exact calculations to see how the infection curve is proceeding and then projecting out different scenarios based on new data. The Yahoo article (and maybe it was the author, not the nobel laureate) seemed oblivious to this fact in the article. Originally Posted by sagegrouse
Same with the commentary on social distancing. The article didn't present any new information, just repackaged what is presented every day as if it were offering some insight. It wasn't.
-
03-23-2020, 01:03 PM #2076
Member
- Join Date
- Feb 2007
Is that similar to my "how many times have I told you" and "I'm always right" which both see heavy rotation in my personal family research lab. Originally Posted by rsvman
Nothing incites bodily violence quicker than a Duke fan turning in your direction and saying 'scoreboard.'
-
03-23-2020, 01:14 PM #2077
 Member
Member
- Join Date
- Mar 2010
- Location
- Cincinnati
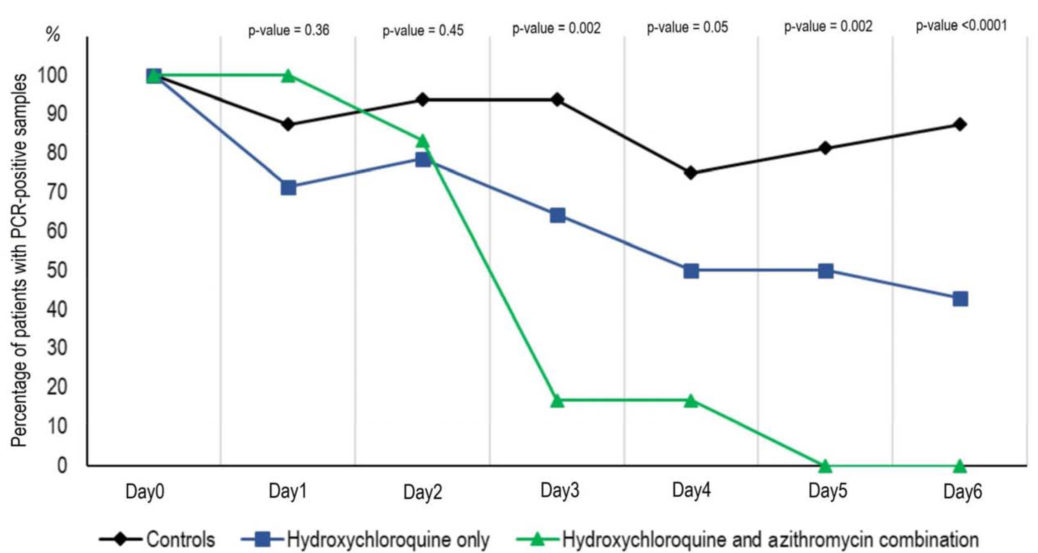
New York Gov. Andrew Cuomo announced Sunday that New York State has acquired 70,000 doses of hydroxychloroquine, 10,000 doses of zithromax and 750,000 doses of chloroquine to implement drug trials to treat patients with coronavirus, which will begin on Tuesday.
Researchers in France recently performed a small study on 30 confirmed COVID-19 patients, treating each with either hydroxychloroquine on its own, a combination of the medicine with the antibiotic, as well as a control group that received neither. Results:
-
03-23-2020, 01:20 PM #2078
Member
- Join Date
- Mar 2007
I'm not a doc and it's not my place to tell you what to do morally or otherwise. A neighbor of ours lost her grandmother in Italy last week due to a heart attack. She had been feeling bad for about a week and knew it was her heart (history of issues), but there were no available cardiologists as it was already "all hands on deck" at the hospitals. Originally Posted by fisheyes
I have absolutely no idea what is the best thing to do, all I can do is offer a prayer for you that you find peace in your decision.
With regards to malpractice, I imagine many things will change for the duration of this emergency and I hope this is one. I know the medical board people loosened up some rules regarding telemedicine. I imagine they will do the same regarding COVID-19 care.
https://www.ncmedboard.org/resources...id-19-concerns
-
03-23-2020, 01:20 PM #2079
Member
- Join Date
- Feb 2007
- Location
- Raleigh
I'm almost exactly in the same situation/predicament. I stopped invasive/interventional work over 1.5 years ago and have about two years "seniority" (aka as geezerhood) on you. I'm in a small group practice that became part of a large group hospital practice about six months ago but our work is still >95% outpatient work and our small group census is usually quite low and our hospital rounds/work quite limited. I'm still committed to inpatient consultations and follow-up on our patients with heart attacks, heart failure, dysrhythmias and abnormal blood pressures, but, since the hospitalists agreed to admit all our patients over 5 years ago and the intensivists manage the ICU patients, we get far less calls than in our earlier years. Bottom line I guess is that I'm well trained and experienced and remain loyal to caring for patients and will work where called/assigned but have some (significant?) reservations about being placed back in an in-patient environment as described above. Originally Posted by fisheyes
[redacted] them and the horses they rode in on.
-
03-23-2020, 01:41 PM #2080
Member
- Join Date
- Mar 2010
- Location
- Cincinnati
Facts about Italy:
- Italy has the oldest population in Europe.
- The average age of those who have died was 81.
- More than 99% of Italys coronavirus fatalities were people who suffered from previous medical conditions.
- As of March 14, South Korea reported that nearly 30% of its confirmed coronavirus cases were in patients ages 20 to 29. In Italy, by comparison, 3.7% of coronavirus patients fell into that age range.
- At the outbreak of the crisis, Germany had 29.2 intensive care beds per 100,000 people, whereas Italy had 12.5.
Similar Threads
-
Masters 2020
By OldPhiKap in forum Off TopicReplies: 175Last Post: 11-20-2020, 09:24 PM -
2020 NBA Playoffs
By cato in forum Elizabeth King ForumReplies: 1349Last Post: 10-17-2020, 11:29 PM -
Coronavirus - those we've lost
By JasonEvans in forum Off TopicReplies: 62Last Post: 05-08-2020, 09:42 PM -
FB: 2020 Schedule is out
By nocilla in forum Elizabeth King ForumReplies: 31Last Post: 01-22-2020, 07:08 PM
 Posting Permissions
Posting Permissions
- You may not post new threads
- You may not post replies
- You may not post attachments
- You may not edit your posts