


 Reply With Quote
Reply With QuoteFinally somebody has given an informed estimate as to when well be able to turn the corner on this thing.
Former Food and Drug Administration Commissioner Scott Gottlieb headed a team that put out a Road Map to Reopening which described when it would be appropriate to move from Phase 1, where we are now. The goal of Phase I is: Slowing the transmission of SARS-CoV-2 across the United States by reducing the effective reproduction number of infections,
Increasing testing capacity to accommodate the ability to test everyone with symptoms and their close contacts, and
Ensuring the health care system has the capacity to safely treat both COVID-19 patients and others requiring care.
They describe the following conditions in order to move to Phase II: A sustained reduction in cases for at least 14 days,
Hospitals in the state are safely able to treat all patients requiring hospitalization without resorting to crisis standards of care,
The state is able to test all people with COVID-19 symptoms, and
The state is able to conduct active monitoring of confirmed cases and their contacts.
The goals of Phase II are to: Lift strict physical distancing measures in a concerted and careful fashion,
Allow the vast majority of businesses and schools to open, and
Continue to control SARS-CoV-2 transmission so we do not revert back to Phase I.
In Phase II, the majority of schools, universities, and businesses can reopen. Teleworking should continue where convenient; social gatherings should continue to be limited to fewer than 50 people wherever possible. Other local restrictions should be considered, such as those that limit people from congregating in close proximity.
Results 2,721 to 2,740 of 22199
-
03-30-2020, 12:03 PM #2721

 Member
Member


- Join Date
- Feb 2007
- Location
- Steamboat Springs, CO
Mine said "Microwave Safe" on top. Originally Posted by Acymetric
Originally Posted by Acymetric
 Sage Grouse
Sage Grouse
---------------------------------------
'When I got on the bus for my first road game at Duke, I saw that every player was carrying textbooks or laptops. I coached in the SEC for 25 years, and I had never seen that before, not even once.' - David Cutcliffe to Duke alumni in Washington, DC, June 2013
-
03-30-2020, 12:04 PM #2722

 Member
Member
- Join Date
- Mar 2010
- Location
- Cincinnati
-
03-30-2020, 12:24 PM #2723
Member
- Join Date
- Oct 2016
- Location
- Texas
Convalescent Serum
Convalescent serum had been mentioned previously in the thread. Houston Methodist has been given the go ahead by the FDA for the procedure. I believe the local news mentioned they had been granted approval to treat 2 patients.
https://finance.yahoo.com/news/fda-a...150200582.html
-
03-30-2020, 12:26 PM #2724
On Holiday
- Join Date
- Feb 2007
- Location
- Deeetroit City
Originally Posted by swood1000
This is WAY too reasonable and well thought out. It has absolutely no chance in today's political climate. I can envision the arguments about how the standards benefit one state, region, party, or demographic over another.
-
03-30-2020, 12:27 PM #2725
Member
- Join Date
- Nov 2014
- Location
- The People's Republic of Travis County
Good news; I really hope this helps! Originally Posted by LegoBatman
-
03-30-2020, 12:28 PM #2726
 Member
Member
- Join Date
- Jul 2008
- Location
- Rent free in tarheels heads
I calculate NC at roughly 18 tests per 10K people. That’s based on Herald-Sun stating nearly 19,000 tests have been performed in NC and taking the population as 10.38M. That puts NC pretty much right in the middle in terms of rate of testing. Originally Posted by PackMan97
Coach said no 3s. - Zion on The Block
-
03-30-2020, 12:30 PM #2727
Member
- Join Date
- Mar 2010
- Location
- Cincinnati
They need to get some of those toaster-sized test machines from Abbot Labs that were just authorized by the FDA. Originally Posted by Bob Green

Apparently they can deliver positive results in as little as five minutes and negative results in 13 minutes. There are currently about 18,000 of these machines in the U.S. and Abbott expects to ramp up manufacturing to deliver 50,000 tests per day.
-
03-30-2020, 12:31 PM #2728
 Member
Member
- Join Date
- Feb 2007
- Location
- New Jersey
Originally Posted by swood1000
Right, let's either go with this ^ or pick a random date out of the air Originally Posted by BD80
") Rich
Rich
"Failure is Not a Destination"
Coach K on the Dan Patrick Show, December 22, 2016
-
03-30-2020, 12:41 PM #2729
Member
- Join Date
- Jul 2008
- Location
- Rent free in tarheels heads
I read about this last week. But its frustrating to keep hearing about all these incremental and new testing capabilities but with no understanding of how, when and where all of this is being deployed around the country. Originally Posted by swood1000
Coach said no 3s. - Zion on The Block
-
03-30-2020, 12:48 PM #2730
Member
- Join Date
- Nov 2007
- Location
- Vermont
Indeed...it's a good idea not because it's a good investment, but rather because it's a good thing to do. Originally Posted by -jk
by the way: in checking in with friends in NYC, I've found that several of them have had the virus (they are quite certain) and lots of their friends have as well, yet almost none of them have been tested, because they didn't get to the point where they required hospitalization...the point being there's a whole lot of it down there, and having enough beds and respirators is likely to become a real issue very very soon...hard to see how they bend that curve.Last edited by budwom; 03-30-2020 at 12:55 PM.
-
03-30-2020, 12:51 PM #2731
Member
- Join Date
- Mar 2007
- Location
- Asheville
Well then, take the extra eight minutes and make them all negative results! Crisis over! Originally Posted by swood1000
-
03-30-2020, 12:57 PM #2732
Member
- Join Date
- Nov 2007
- Location
- Vermont
yeah, there's been a guy on the news talking about ramping up his company's ventilator production, but the numbers are really small...like a few thousand this month, 3k the next, does not appear to be sufficient for the near term crisis... Originally Posted by Dr. Rosenrosen
-
03-30-2020, 01:02 PM #2733
Member
- Join Date
- Jul 2008
- Location
- Rent free in tarheels heads
Hoping that someone somewhere is coordinating all these efforts but Im not holding my breath. Sounds more like governors making one-off efforts to purchase what they need if they can get it. I hope thats wrong. Originally Posted by budwom
Coach said no 3s. - Zion on The Block
-
03-30-2020, 01:23 PM #2734
Member
- Join Date
- Mar 2010
- Location
- Cincinnati
Apparently, the Abbott machines use isothermal nucleic acid amplification technology instead of PCR, and so do not require the time-consuming series of alternating temperature cycles. Does this mean that PCR is becoming old technology? Originally Posted by rsvman
-
03-30-2020, 01:45 PM #2735
Member
- Join Date
- Feb 2007
- Location
- Cincinnati, Ohio
For the more senior members of the board, you'll remember that back in the day we could have just built a tester at home and gotten this straightened out much more quickly.
Heathkit.jpg
But times have changed.
OK, back to the important stuff - hope somebody can crank out these new kits post haste.
-
03-30-2020, 02:05 PM #2736
 Member
Member
- Join Date
- Feb 2007
- Location
- Durham, NC
Well, I didn't think of myself as "more senior", but now I do. My dad and his friend built our first color TV from Heathkit. Originally Posted by Ggallagher
-
03-30-2020, 02:13 PM #2737
On Holiday
- Join Date
- Feb 2007
- Location
- Deeetroit City
There is no "L" in "Heathkit!" Originally Posted by Ggallagher
FWIW: I was building my Dynakit pre-amplifier the night I won the tickets to the limited preview of "Star Wars" in May of 1977. I feel like I could build a few Covid tests kits at home now.
I've got time.
-
03-30-2020, 04:01 PM #2738
Moderator
- Join Date
- Feb 2007
- Location
- Norfolk, VA
Governor Northam has issued a Stay at Home order for Virginia:
https://www.wavy.com/news/health/cor...-for-virginia/Bob Green
-
03-30-2020, 04:22 PM #2739
Member
- Join Date
- Mar 2010
- Location
- Cincinnati
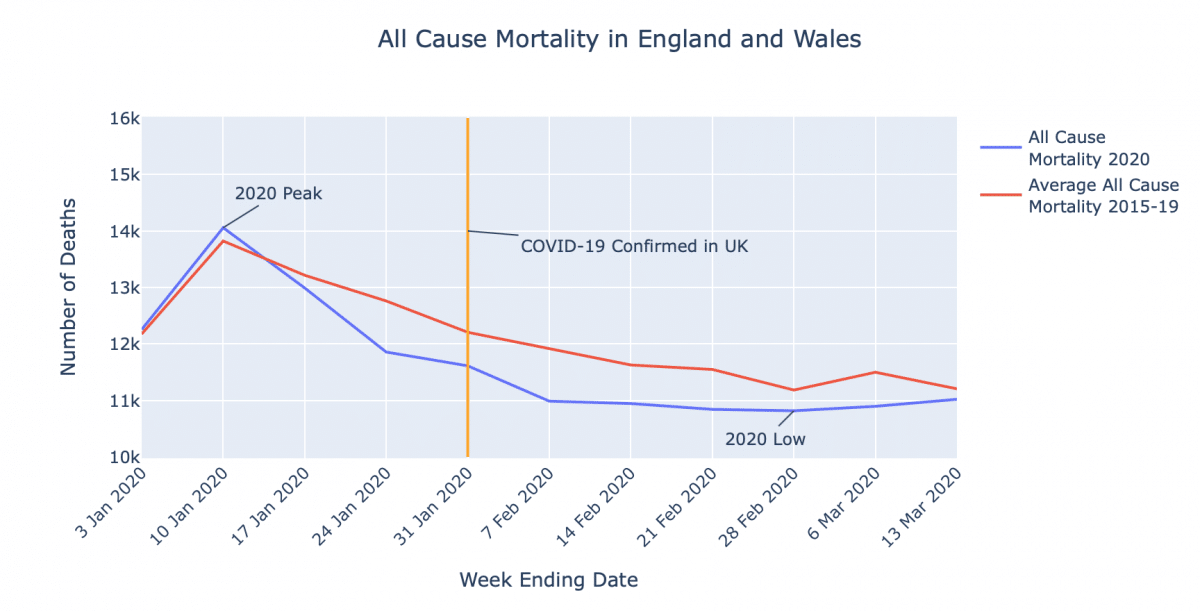
Apparently, when flu deaths in a year are listed, the number given is the number of deaths over and above what one would expect to happen in that year (at least in the UK). This is because quite a few of these people would have died anyway of old age or of other health conditions. So a way exists to estimate these “excess deaths” from flu. However, with Covid-19 this reduction is not made and we are given the gross death number. Consequently the number of deaths attributed to Covid-19 is inflated.
In Great Britain, 600,000 people die each year. Neil Ferguson, the Imperial College London scientist whose recent research on Covid-19 received much press, now is expecting 20,000 deaths or fewer, and says that half to two thirds of those people would have died anyway before the end of the year “because these are people at the end of their lives or who have underlying conditions.”
One British statistician says that if the number can be kept to 20,000 by stringent suppression measures there may end up being a minimal impact on overall mortality for 2020 (although background mortality could increase due to pressures on the health services).
All-cause mortality in England and Wales in 2020 compared to prior years is below (the Office for National Statistics only lists 2020 up to March 13).
-
03-30-2020, 05:13 PM #2740
 Member
Member
- Join Date
- Feb 2007
Has anyone called Elizabeth Holmes and asked her to produce a test?
My Quick Smells Like French Toast.
Similar Threads
-
Masters 2020
By OldPhiKap in forum Off TopicReplies: 175Last Post: 11-20-2020, 09:24 PM -
2020 NBA Playoffs
By cato in forum Elizabeth King ForumReplies: 1349Last Post: 10-17-2020, 11:29 PM -
Coronavirus - those we've lost
By JasonEvans in forum Off TopicReplies: 62Last Post: 05-08-2020, 09:42 PM -
FB: 2020 Schedule is out
By nocilla in forum Elizabeth King ForumReplies: 31Last Post: 01-22-2020, 07:08 PM
 Posting Permissions
Posting Permissions
- You may not post new threads
- You may not post replies
- You may not post attachments
- You may not edit your posts